How Much Protein Do You Actually Need on a GLP-1?
Why eating less doesn’t mean you’re eating right


When I started Ozempic, I thought the hard part would be the nausea. It was not. The hard part was figuring out how to eat enough protein when the idea of food was a “turn off”.
Here’s the problem with GLP-1 medications and protein: they work by suppressing your appetite, sometimes dramatically. That sounds like a win — and for weight loss, it is. But your body doesn’t just burn fat when you’re eating very little. It burns muscle too. That sounds manageable in your 30s. At 50-plus, it’s a different story.
Except that after 50, we’re already fighting a condition called sarcopenia — the natural, age-related loss of muscle mass that starts in your 40s and accelerates every decade. Add a GLP-1 medication and a dramatically reduced appetite to that picture, and you have a real problem: you’re losing weight, but some of what you’re losing is muscle you cannot easily get back.
The research on this is still emerging, but what we know is sobering. A 2023 study in the journal Obesity found that people on semaglutide lost a significant portion of their weight as lean mass — not just fat. For older adults already at risk for sarcopenia, that’s not a side effect to brush off. It affects how you move, how you feel, your balance, your independence.
This is not a reason to avoid GLP-1 medications. They work. But it is a reason to be deliberate about protein.
So how much protein do you actually need?
The standard recommendation — 0.8 grams per kilogram of body weight — was set decades ago and is widely considered too low for older adults, especially those losing weight. It’s a floor, not a target.
You’ve probably heard “1 gram per pound of body weight” from fitness influencers. That’s on the high end, and not necessarily supported by the research for non-athletes. But the evidence does support eating more than the baseline — especially when you’re over 50 and losing weight.
More recent research — including guidance from the European Society for Clinical Nutrition and Metabolism (ESPEN) — recommends that older adults aim for 1.0 to 1.2 grams of protein per kilogram of body weight per day, with higher amounts (up to 1.5 g/kg) recommended for those who are ill, injured, or actively trying to preserve muscle during weight loss.
The American College of Sports Medicine lands in a similar place for active older adults: 1.0 to 1.6 g/kg/day depending on activity level and goals.
For me, at 200 pounds (about 91 kg), that translates to roughly 91 to 136 grams of protein per day — on a day when I might only feel like eating once or twice.
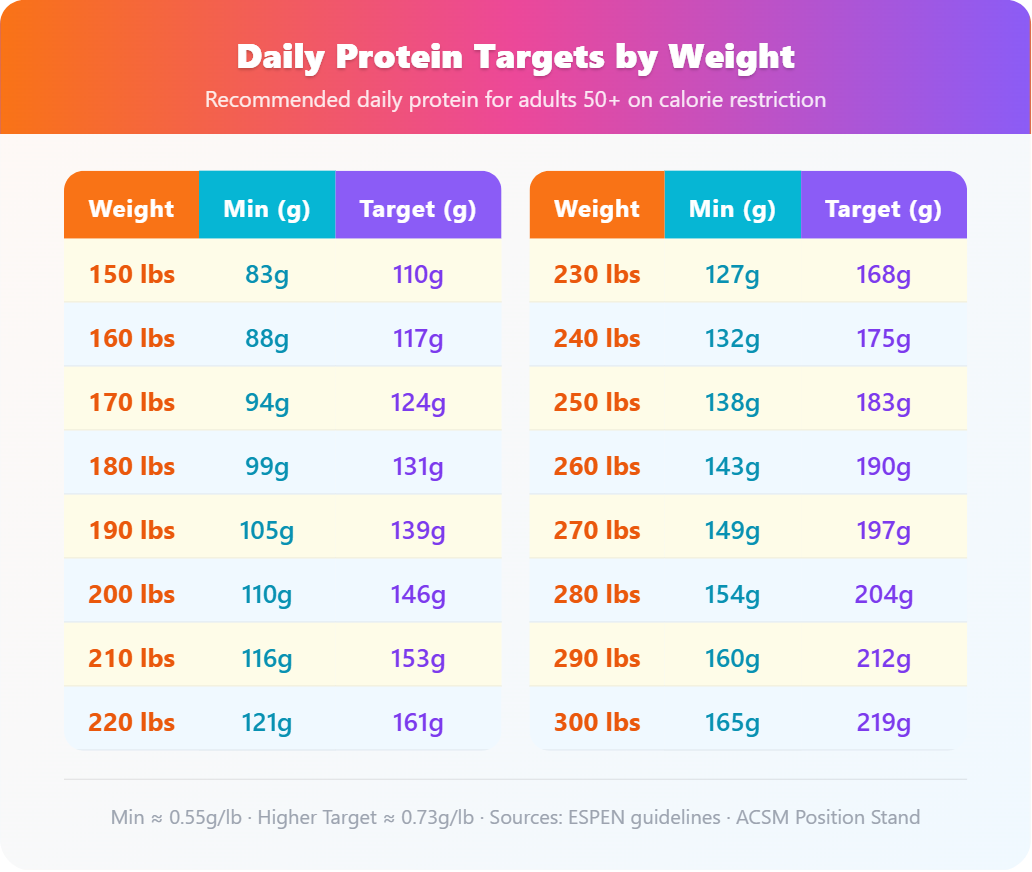
Your protein target by weight
Use this table to find your daily protein range. The minimum column reflects adequate intake for older adults on calorie restriction. The higher target supports active muscle preservation — something worth aiming for on a GLP-1.
What this looks like in real food
Getting 100 grams of protein in a day when you’re not hungry is genuinely hard. A large egg has about 6 grams. A 3-ounce serving of chicken breast has about 26 grams. Greek yogurt runs around 17 grams per serving. You’re doing math at every meal.
The foods that help most are the ones that are protein-dense without requiring much volume: eggs, cottage cheese, Greek yogurt, canned fish, chicken thighs, edamame. Protein shakes can fill gaps — not as a replacement for food, but as a backup when eating feels impossible.
The practical reality is that most people on GLP-1s eat far less protein than they need, not because they don’t know better, but because the appetite suppression makes it feel unnecessary. You’re not hungry. You’re losing weight. Everything seems fine. Until it isn’t.
Spreading protein across meals matters too. Your body can only use so much at once for muscle synthesis — research suggests around 25 to 40 grams per meal is the sweet spot. Eating 80 grams at dinner and skipping it all day doesn’t give you the same muscle-preserving benefit as distributing it more evenly.
I monitor my protein every day now. Not obsessively, but intentionally. It’s one of the few things I can control in a process that often feels like it’s running me rather than the other way around.
The medication does the heavy lifting on appetite and blood sugar. My job — the part I can actually manage — is making sure that when I do eat, I’m eating the right things. Protein first. Always.
Sources and further reading
Examine.com: Protein Intake Evidence Guide — examine.com/guides/protein-intake/
ESPEN guidelines on clinical nutrition and aging (2022 update)
Wilkinson et al. (2023): Lean mass loss during semaglutide treatment in adults with obesity, Obesity journal
American College of Sports Medicine Position Stand on protein and exercise